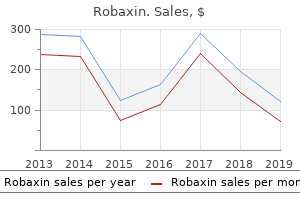
"500 mg robaxin with visa, muscle relaxant nerve stimulator."
By: Michael A. Gropper, MD, PhD
- Associate Professor, Department of Anesthesia, Director, Critical Care Medicine, University of California, San Francisco, CA

https://profiles.ucsf.edu/michael.gropper
However gut spasms discount robaxin 500 mg line, it can occur spasms with fever buy robaxin 500 mg on-line, particularly in the sigmoid colon if the mesentery is quite long spasms in upper abdomen order robaxin 500mg without prescription, particularly after pelvic operations. The majority of patients with constipation and a dilated rectum and/or colon at proctosigmoidoscopy or barium enema have idiopathic or acquired megarectum. These patients can often present in childhood (many of them presenting with encopresis) and in the elderly with a fecal impaction. The cause of the megarectum is unknown, but if the onset is in childhood it may be the result of chronic stool holding by the child, leading to progressive distention of the rectum and eventual loss of awareness of rectal distention. Once this has occurred the child can no longer recognize when stool is present in the rectum. The distention of the rectum causes chronic inhibition of the resting tone of the internal anal sphincter. This leads to the loss of control of liquid or semisolid stool that passes by the fecal impaction without the patient being aware of it. The distal colon remains contracted due to this loss of neurons, and the inability to dilate, whereas the normal proximal colon dilates as it fills with stool. Most of these patients present early in life with constipation and colonic obstruction, and require surgery. However, a few patients have a very short segment of denervated distal colon, so that they can overcome the obstruction by forcing stool out of the rectum. Anorectal manometry, will demonstrate an abnormal rectoanal inhibitory reflex (Figure 9). However, a definite diagnosis requires deep rectal biopsy from the denervated segment, which will show absence of the myenteric plexus ganglion cells and hypertrophy of nerve fiber bundles. These patients will also have an absent rectoanal inhibitory reflex if the disease involves the rectal myenteric plexus. Shaffer 370 this section will review the symptoms associated with anorectal pathology, and the techniques of anorectal examination. History As in most of medicine, taking a careful history is the most productive step in leading to a diagnosis. In the evaluation of the patient with anorectal complaints, there are a limited number of questions to be asked. Pain There are three common lesions that cause anorectal pain: fissure in ano, anal abscess, and thrombosed external hemorrhoid. If the pain is sharp, and occurs during and for a short time following bowel movements, a fissure is likely. Continuous pain associated with a perianal swelling usually stems from thrombosis of perianal vessels, especially when there is an antecedent history of straining, either at stool or with physical exertion. The absence of an inflammatory mass in the setting of severe local pain and tenderness is typical of an intersphincteric abscess. The degree of tenderness usually prevents adequate examination, and evaluation under anesthesia is necessary to confirm the diagnosis and to drain the pus. Tenesmus, an uncomfortable desire to defecate, is frequently associated with inflammatory conditions of the anorectum. Although anal neoplasms rarely produce pain, invasion of the sphincter mechanism may also result in tenesmus. Anorectal pain is so frequently, and erroneously, attributed to hemorrhoids, that this point bears special mention: pain is not a symptom of uncomplicated hemorrhoids.
Diseases
- Acute tubular necrosis
- Systemic carnitine deficiency
- Achromatopsia
- Aortic coarctation
- Zinc toxicity
- Adrenal adenoma, familial
It is unlikely that if the patient completed the pulmonary rehabilitation course originally and failed to muscle relaxant veterinary buy cheap robaxin 500mg on-line gain a benefit muscle relaxant uk purchase robaxin 500 mg otc, they would benefit a second time round muscle relaxant medicines buy cheap robaxin 500mg, unless circumstances such as an exacerbation interrupted the initial programme. Pulmonary rehabilitation is not suitable for people with unstable cardiac disease, locomotor or neurological difficulties precluding exercise such as severe arthritis or peripheral vascular disease, and people in a terminal phase of an illness or with significant cognitive or psychiatric impairment. Aetna considers entry into a medically supervised outpatient pulmonary rehabilitation program medically necessary when all of the following criteria are met: i. Member has a reduction in exercise tolerance that restricts the ability to perform activities of daily living and/or work; and iv. Member does not have a recent history of smoking or has quit smoking for at least 3 months; and vi. Member has a moderate to severe functional pulmonary disability as evidenced by either of the following: 1. Member is physically able, motivated and willing to participate in the pulmonary rehabilitation program and be a candidate for self-care post program; and viii. Member does not have any concomitant medical condition that would otherwise imminently contribute to deterioration of pulmonary status or undermine the expected benefits of the program. Aetna considers pulmonary rehabilitation medically necessary for persons receiving a medically necessary lung transplantation c. However, exceptions may be made for patients undergoing a repeat pulmonary rehabilitation program in connection with lung transplantation or lung volume reduction surgery. Aetna considers pre-operative pulmonary rehabilitation in persons undergoing surgery for lung cancer experimental and investigational because the effectiveness of this approach has not been established. According to available guidelines, persons with very severe pulmonary impairment are not appropriate candidates for pulmonary rehabilitation. A typical course of pulmonary rehabilitation extends for up to 6 weeks or 36 hours of therapy. Coverage of pulmonary rehabilitation may be subject to applicable limits on short-term rehabilitation. There is mixed or insufficient evidence of effectiveness for decreasing hospitalizations and improving mortality. Most expert guideline and other payer policies recommend pulmonary rehabilitation for moderate or severe respiratory disease for patients without severe comorbid conditions or who are not housebound. Pulmonary rehabilitation must be a multidisciplinary program including exercise and education. Repeat pulmonary rehabilitation programs should be limited to those patients who successfully completed a previous program more than one year prior, particularly if that patient has lung surgery; although there is no evidence of benefit of repeat programs. G0237 (Therapeutic procedures to increase strength or endurance of respiratory muscles, face to face, one on one, each 15 minutes (includes monitoring)) ii. G0239 (Therapeutic procedures to improve respiratory function or increase strength or endurance of respiratory muscles, two or more individuals (includes monitoring)) iv. S9437 (Pulmonary rehabilitation program, non-physician provider, per diem) are on the Ancillary Procedures File. Pulmonary rehabilitation is only covered for 1) A multidisciplinary program with includes supervised exercise therapy, patient education, and smoking cessation (if applicable). Repeat pulmonary rehabilitation programs should be limited to those patients who successfully completed a previous program more than one year prior and who have had a significant change in their health status. In addition, blood lead level screening of any child between ages 24 and 72 months with no record of a previous blood lead screening test is indicated. Pulmonary rehabilitation is currently is on multiple lines on the Prioritized List with no limitations on coverage. Pulmonary rehabilitation is a multi-disciplinary treatment that might include exercise training, nutritional counseling, education, breathing strategies, psychological counseling, etc. Longer pulmonary rehabilitation programs (beyond 12 weeks) produce greater sustained benefits than shorter programs.
Quality 500mg robaxin. Pain Relief Cream by Dr. Pat - Topical Analgesic Gel - Icy and Hot Therapy - Muscle & Arthritis Pain.
Multidisciplinary user meeting Multidisciplinary user meetings are obligated to muscle relaxant generic order robaxin 500mg without a prescription define hospital policies about minimally invasive surgery and to spasms left side purchase 500mg robaxin with mastercard secure standards of quality spasms back buy robaxin 500 mg with amex. These meetings should include: Registration and training of the surgical team Training facilities Introduction of new materials and techniques Maintenance of uniformity in material and techniques Evaluation of safety and care quality Applicable guidelines, standards, and laws the underestimated risks of minimally invasive surgery. The meetings should include the following items: There should be a formal procedure for introducing new instruments, equipment, and techniques There should be relevant maintenance procedures and medical equipment checks the hospital should evaluate outcomes, incidents, and complications, and it should provide regu lar annual reports evaluating all laparoscopic procedures carried out. The hospital management should evaluate the management of certification and accreditation where ap plicable and according to the standards of practice of the national and international professional societies and regulatory bodies. General and specific complications Oncological and functional outcomes, as well as the number and severity of complications, determine the quality of the surgery. The categorization of complications in the Clavien-Dindo classification system is ac cepted internationally (Table3. The Clavien-Dindo classification system de fines a complication as any deviation from the expected postoperative course. Problems solved during surgery are not mentioned in this complication registration system. The international Clavien-Dindo classification system for surgical complications Grade Definition I Any deviation from the expected postoperative course without any need for intervention such as pharmacological, radiological, of surgical treatment. The registration of complications may be useful for benchmarking with other organizations for the purpose of improving the quality of care. Complications, outcome registration, and guidelines Complications in surgery are important causes of morbidity and mortality, and may result in an increased length of hospital stay, repeat surgery, additional medical treatment, legal issues, and increased costs. Making the out comes public promotes transparency, which in turn helps patients, policy makers and healthcare insurers make decisions. Training and certification John Rietbergen, Carl Wijburg, Barbara Schout, Henk van der Poel, Ben Knipscheer, Irene Tjiam, Nicole Dreessen, Willem Brinkman, Jean-Paul van Basten 4. Introduction Many urology trainees have reported underexposure to formal training for laparoscopic skills in a survey among European trainees. Practical training leading to certification While some skills are best learned in a clinical environment, a skills laboratory is probably the best learning environment for other skills. Some of these skills can only be acquired in a very realistic situation, while others, like using surgical instruments and changing gears, can easily be taught outside the realistic environment. The certification is actually an approval of the mastery of laparoscop ic and robotic skills. However, such organizations rely on profes sional societies, such as the Royal College of Surgeons and the American College of Surgeons. These societies provide an educational curriculum that includes training and testing before certification. Outline of a module of the Dutch program on urological practical skills 34 Recommendations in laparoscopic and robotic surgery in urology 4. The tests are set up in a box with an endoscope and a light source connected to a screen. The examinee can practice for 1 minute to get used to the instruments and the task. Lift each object with a grasper in your non-dominant hand and transfer it to the dominant hand. Once all objects have been transferred, transfer them back to the original side in the reverse proce dure. Grasp the object with your dominant hand and transfer it to your non-dominant hand. Place each object on a peg on the original side of the board with your non-dominant hand. Each transfer must be done in mid-air, without the use of the pegs or block for assistance.
Lobelie (Lobelia). Robaxin.
- Are there safety concerns?
- What is Lobelia?
- Are there any interactions with medications?
- Smoking cessation.
- Dosing considerations for Lobelia.
- How does Lobelia work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96260
References:
- http://www.infohep.org/v634934198457870000/file/1185549/HIV_Curriculum.pdf
- https://www.idsociety.org/globalassets/idsa/topics-of-interest/antimicrobial-resistance/foar-report-1-up-final-1.pdf
- https://tba.com/pdf/nailbafldundguide_tba.pdf
- http://samples.jbpub.com/9781284103960/Chapter1.pdf
- http://downloads.hindawi.com/journals/bmri/2014/354906.pdf